Research Articles & Studies
Research Articles & Studies
Home » Research
Uncover the groundbreaking science behind the DISCSEEL® Procedure.
Studies have demonstrated the clinical efficacy of the DISCSEEL Procedure in treating disc-related pain.
Latest Study Abstract
Long-term Investigation of Annulargrams and Intra-annular Fibrin to Treat Chronic Discogenic Low Back Pain and Radiculopathy: 1-, 2-, and 3-Year Outcome Comparisons of Patients with and without Prior Surgery
Authors: Kevin Pauza, MD , Kwadwo Boachie-Adjei, BS , Patrick Ercole, PhD , Francis Hussey, IV, MS , Joseph Nguyen, MPH , Akua Serwaa-Sarfo, MPH , Jacob Sutton, MD , Carrie Wright, MD, MS , William Delany Murrell, MD, MS
MANUSCRIPT NUMBER:
PAINPHYSICIAN-D-23-00261R1
FULL TITLE:
Long-term Investigation of Annulargrams, Intra-annular Fibrin Treat Chronic Discogenic LBP-Radiculopathy: 1-3 Year Outcomes Comparisons Patients with and without Prior Surgery
KEYWORDS:
low back, radiculopathy, fibrin, disc herniation, degenerative disc, regenerative, annulargram, annulogram
CORRESPONDING AUTHOR’S INSTITUTION:
Infohealth LLC
BACKGROUND:
Discogenic chronic low back pain (cLBP) and radiculopathy are most prevalent causes of disability worldwide. Prior spine treatments often lack reliability and are associated with adverse events. Among surgical treatment options, discectomies weaken discs to cause accelerated degeneration, and fusions directly cause damaging forces against adjacent discs accelerating their degeneration. Other regenerative
medicine treatments including “stem cell” centrifuged bone marrow aspirate (BMC),and Platelet-Rich Plasma (PRP), lack fibrin’s bio-adhesive properties. Specifically, fibrin is a strong bio-adhesive and it immediately integrates into disc defects and binds,
becomes part of the disc to facilitate new disc tissue growth.
OBJECTIVES:
Evaluate the safety and efficacy of this new pragmatic algorithm which both diagnoses and treats chronic low back pain by (i) identifying Annulus Fibrosus tears (fissures) region of symptoms, and (ii) treating those tears with fibrin, sealing them and facilitating new tissue growth.
STUDY DESIGN:
Retrospective cohort study that prospectively reported validated Powered by Editorial Manager® and ProduXion Manager® from Aries Systems Corporation measures in a registry.
SETTING:
Private, single center, specialized, interventional pain management institution
METHODS:
Subjects suffer with cLBP with or without radiculopathy for greater than six months. Prior to enrollment, all subjects underwent physical therapy and at least four invasive treatments without relief. Failed treatments included BMC or PRP injections, intradiscal or intra-articular into zygapophyseal joints, or combinations of both.
Additional failed treatments included fluoroscopically guided epidural corticosteroids or PRP, or Medial Branch radiofrequency neurotomies. Diagnostic certainty of underlying condition was confirmed by screening MRIs (1.5T) and plain-film radiographs
performed six months prior to treatment and confirmed in 100% of patients enrolled, without concomitant conditions: (i) carcinoma, (ii) fracture, (iii) instability, or (iv) severe vertebral canal or intervertebral foramen stenosis.
OUTCOMES ASSESSMENT:
Oswestry Disability Index (ODI), Low Back and Leg Pain Visual Analog Scale (VAS), PROMIS Global Mental Health (GMH), Estimated Utility Score (EuroQol), and Modified North American Spine Society (NASS) Patient Satisfaction Survey.
RESULTS:
Significant Improvement was demonstrated at 1-, 2-, and 3-years post treatment in all outcomes measures. Mean duration of low back pain prior to treatment was 11.2 years. Subject mean age 56 years, 30% female, 70% male. Both the failed surgery cohort and non-surgery cohort demonstrated significant improvement after fibrin treatment, with the failed surgery cohort realizing greater relative improvement. Significant Improvements in ODI, VAS, and PROMIS (Mental and Physical) were consistent across age, gender, co-morbidity and exposure status. At 12-month follow up, 50% of subjects achieved MCID utilizing ODI. No severe adverse events were reported.
LIMITATIONS:
Limitations include patient demographic factors, outcome-measure sensitivity, or that outcomes were reported prospectively and calculated retrospectively as 1-, 2-, and 3-year timeframes were attained. Although categorical analyses comparing prior surgical with non-surgical cohort was performed, pre-enrollment treatments were not categorized for comparison.
CONCLUSIONS:
Intra-annular fibrin bio-adhesive sealant demonstrates ability as an effective treatment to alleviate discogenic cLBP and radiculopathy for at least three years, even in subjects who all failed multiple prior treatments, including discectomy, fusion, disc PRP or BMC. Results suggest benefit of fibrin sealant; however, future investigations to consider include a randomized double-blind controlled trial and further categorical analyses.
Previous Clinical Research Studies
Original Research Article (Abstract) Intradiscal Injection of Fibrin Sealant for the Treatment of Symptomatic Lumbar Internal Disc Disruption: Results of a Prospective Multicenter Pilot Study with 24-Month Follow-Up
Authors: Way Yin, MD, Kevin Pauza, MD, Wayne J. Olan, MD, Jeff F. Doerzbacher, MS, and Kevin J. Thorne, PhD
BACKGROUND:
Chronic low back pain is the most common cause of disability worldwide, and to date, no surgical or non-surgical treatment has been shown to reliably provide relief in treating chronic low back pain. Lumbar discs are the most common cause of chronic low back pain, and so this investigation evaluates the safety and efficacy of using non-autologous fibrin, introduced intra-annularly, to treat annular defects causing chronic low back pain. Annulargram™ is a dynamic test, identifying annular defects and contrast flow patterns within the 22-25 annular layers. Annulargram™ possess greater sensitivity than does MRI in identifying annular defects, and this dynamic test is somewhat analogous to coronary arteriograms, another dynamic test initially fraught with skepticism before it’s widespread acceptance which changed the paradigm evaluating CAD. Favorable results of ongoing investigations suggest that Annulargram™ will be a mainstay in treating spine pathology. Previous published in vivo investigations demonstrate fibrin’s ability to mechanically repair annular defects and stimulate new disc growth, returning all disc biochemical and mechanical properties to normal. This investigation evaluates the amalgam of refinements meant to improve clinical outcome.
PURPOSE:
To evaluate the safety and efficacy of intra-annular fibrin to treat chronic low back pain. Compared to many prior investigations, this investigation evaluates the amalgam of diagnostic and therapeutic refinements meant to improve patient outcomes, including: (1) Diagnostic Annulargram™ used to identify annular defects; (2) Targeting fibrin to those Annulus Fibrosus defects; and (3) Treating each disc in the region of symptoms. of Subjects were treated by the Principle Investigator, and subjects prospectively reported their outcome measures in the Non-surgical Orthobiologics Registry (ROR). Outcome tools measured; pain, physical function, mental health, quality of life, satisfaction, and adverse events, to evaluate the safety and efficacy of intra-annular non-autologous fibrin in treating patients with moderate to severe chronic low back pain.
STUDY DESIGN:
Prospectively reported outcome measures analyzed retrospectively in the ROR.
PATIENT SAMPLE:
Subjects suffering from low back pain, with or without leg pain, for greater than six months duration, who failed prior treatments, including; intra-discal stem cell or precursor cell injections (BMAC), as well as intra-discal PRP, zygapophyseal joint (facet joint) “stem cell or PRP injections,” physical therapy, fluoroscopically-guided transforaminal or interlaminar epidural injections of corticosteroid, radiofrequency neurotomy, or medial branch blocks to rule out posterior element pain. Several subjects failed to experience relief following surgical discectomy and fusion.
OUTCOME MEASURES:
VAS low back; VAS leg; Numeric Rating Scale (NRS); Bodily Pain; Estimated Utility Score; PROMIS Global Mental Health; Global Physical Health; NASS Patient Satisfaction Index Score; Oswestry Disability Index (ODI); and EuroQuol.
METHODS:
320 Subjects with chronic low back pain (LBP) who failed to experience relief following prior spine treatments underwent a screening lumbar MRI and x-ray. Patients without severe vertebral canal stenosis or spinal instability, as determined by lumbar MRI and lateral X-ray, respectively, were enrolled in this investigation. All subjects reported their pre-treatment outcome measures in the ROR, and then underwent diagnostic Annulograms™, with subsequent intra-annular injection of non-autologous fibrin to treat annular defects of all morphologically abnormal intervertebral discs in the region of symptomology. Subjects reported their pre- and post-treatment outcome measures beginning in 2017 to present, assessing; pain, physical function, mental health, quality of life, and patient satisfaction.
RESULTS:
Statistically significant improvement was realized in every outcome tool comparing baseline to; 3-months, 6-months, and 1-year post-treatment. No subject was lost to follow-up or withdrawn, and no subject experienced an adverse event. The results of the longitudinal analysis demonstrated statistically significant improvement in all outcomes measured. Table ______ [js1] reports the findings of the multiple pairwise comparisons between each time point. The values in each square of the matrix are the Bonferroni-adjusted p-values for each pairwise comparison.
CONCLUSIONS:
Patients with chronic low back pain underwent diagnostic Annulargram™ to identify disc annular defects, and those defects were repaired using intra-annular injection of non-autologous fibrin. Subjects prospectively reported statistically significant improvement of all outcomes at; 3, 6, and 12 months post-treatment, with no adverse events.
Intra-annular Fibrin Discseel®
Intra-annular Fibrin Discseel®
Kevin Joseph Pauza, Maxim Moradian, and Gregory Lutz







Treatment of annular disc tears and “leaky disc syndrome™” with fibrin sealant
Kevin Pauza MDa,b , Carrie Wright BSa,b, , Adam Fairbourn BSa,b
- a Texas Spine and Joint Hospital, 1814 Roseland Blvd, Tyler, Texas 75701
- b Manhattan Spine and Joint Institute, New York City, New York 10128
Available online 24 November 2016, Version of Record 14 December 2016.
Abstract
The surfaces of annulus fibrosus tears are known harbingers of inflammatory constituents within intervertebral discs, stimulating sensitized nocioceptors within those tears. Other current treatment options of internal disc disruption neglect to specifically address the surface of these tears.
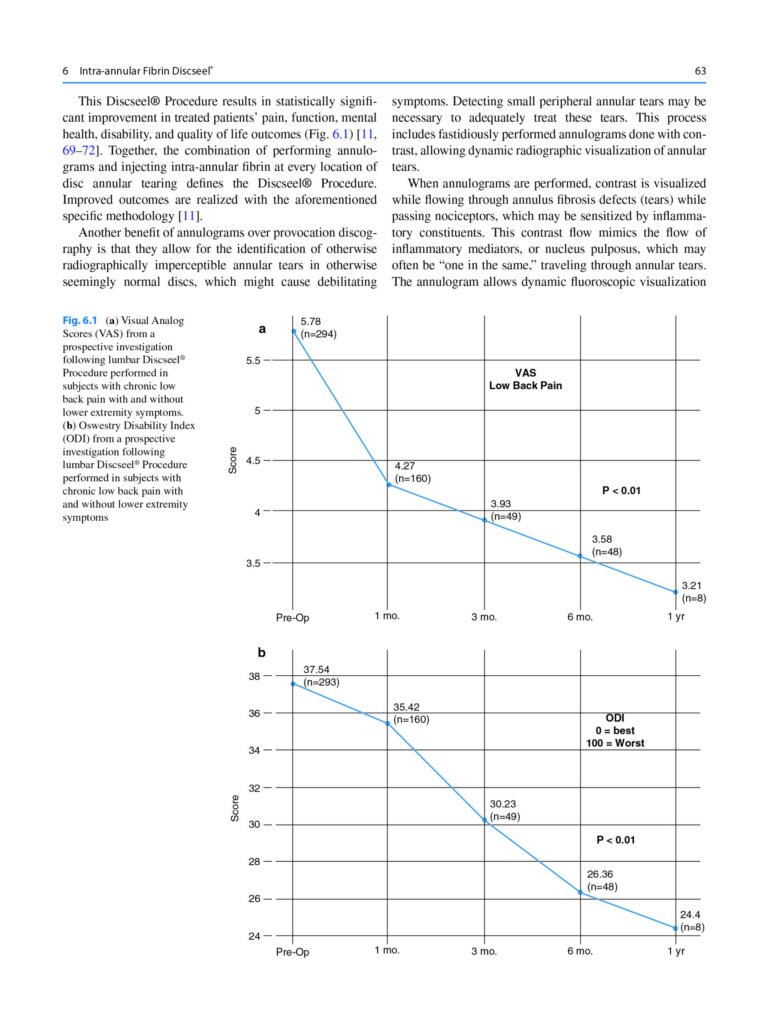
Therefore, this investigation answers the question: does nonautologous fibrin sealant applied to the surface of annulus fibrosus tears mechanically glue and seal annular tears? Regarding this query, results suggest nonautologous concentrated fibrin successfully seals annulus fibrosus tears with a “suture-like mechanical sealant,” serving as a safe option for treating symptomatic or nonsymptomatic intervertebral disc tears. Sealing tears prevents pain-generating chemicals of the nucleus pulposus from leaking through annular tears. More specifically, fibrin sealant minimizes or eliminates extravasation of nucleus pulposus through tears and voids within the annulus fibrosus. Moreover, an investigation subjecting discs to an “internal pressure challenge” objectively affirms fibrin׳s ability to seal torn and degenerated discs against a pressure challenge. (1 psi = 6.89476 kPs (disc mean pressure pretreatment = 75.84 kPs; post-treatment = 179.3 kPs: (n = 347, P < 0.001). Therefore, sealing annular tears serves to minimize extravasation of nucleus pulposus through annular tears, thus potentially treating symptoms caused by internal disc disruption, “Leaky Disc Syndrome™,” and chemical radiculopathy. Additionally, sealing annular tears potentially allows adjunctive regenerative biologics such as mesenchymal precursor cells, platelet rich plasma, and growth factors to remain within discs, thus, potentially optimizing their efficacy. A prior in vivo investigation demonstrated the vast majority of mesenchymal stem cells leaked from animal intravertebral discs, and another demonstrated radiolabeled mesenchymal stem cells leaked from degenerated discs and were subsequently found within new exuberant osteophytes adjacent to the degenerated disc. Intra-annular nonautologous concentrated fibrin shares a benefit of other intradiscal biologics in that fibrin does not cause aberrant detrimental mechanical forces on adjacent discs, compared with surgical fusion and disc arthrodesis, which both cause aberrant, potentially damaging mechanical forces on adjacent segments. The mean number of morphologically abnormal lumbar intervertebral discs in this population with chronic low back pain was 3.21 discs.
Fibrin sealants in lumbar annuloplasty after endoscopic discectomy as a method to prevent recurrent lumbar disc herniation
PMID: 32782757
Author(s):
Pooya Torkian, ORCID iD: 0000-0001-6147-8145,1
Keivan Daneshvar, ORCID iD: 0000-0002-0345-0379,2
Ebrahim Taherian, ORCID iD: 0000-0003-4942-4528,3
Yasaman Rezaeifar, ORCID iD: 0000-0001-6535-5062,4
Shahram Akhlaghpoor3
Abstract:
Fibrin sealant as a promising agent for providing scaffold and efficient hemostasis is widely accepted in several specialties. However, the outcome of Fibrin sealants in lumbar annuloplasty after endoscopic discectomy has not been evaluated in patients with disc herniation. The goal of this study was to evaluate the efficacy, response, and probability of future recurrence rates in herniated nucleus pulposus (HNP) with the use of fibrin sealant in conjunction with endoscopic disc surgery. A total of 35 patients (28 men, 7women) were evaluated, including 18 patients who underwent endoscopic discectomy alone and 17 patients that received fibrin sealant at the site of annulus tear and endoscopic discectomy. All patients were followed through both clinical and imaging methods for an average of 10.5 months. Primary outcome measure was defined as lumbar decompression approved by imaging and symptom alleviation after endoscopic spinal discectomy with Visual Analogue Scale (VAS) score ≤ 4 (cut-off point). Median size of annular tearing was significantly lower in the endoscopic discectomy group (median, 3) (minimum, 2; maximum, 5); however, the corresponding factor in the endoscopic discectomy plus fibrin sealant group was significantly larger (median, 6) (minimum, 5; maximum, 10), with P <0.001. Only one patient in the endoscopic discectomy group had an HNP recurrence during follow-up compared to two patients in the endoscopic discectomy plus fibrin sealant group. Due to the temporary effects of fibrin sealant in preventing disc herniation and the observed recurrence rate in both the case and control groups, the results of this study suggest a role of fibrin sealants combined with endoscopic discectomy to prevent early HNP recurrence rate.
Keywords:
Fibrin sealant, endoscopic discectomy, disc herniation
Biological and biomechanical effects of fibrin injection into porcine intervertebral discs
Spine (Phila Pa 1976) . 2011 Aug 15;36(18):E1201-9. doi: 10.1097/BRS.0b013e31820566b2.
Affiliations: Department of Orthopaedic Surgery, University of California, San Francisco, CA, USA.
- PMID: 21325992
- DOI: 10.1097/BRS.0b013e31820566b2
Abstract
STUDY DESIGN: Surgically denucleated porcine intervertebral discs (IVD) were injected with BIOSTAT BIOLOGX Fibrin Sealant (FS), and the in vivo effects were assessed over time by histological, biochemical, and mechanical criteria.
OBJECTIVE: The objectives were to test whether the intradiscal injection of FS stimulates disc healing.
SUMMARY OF BACKGROUND DATA: Disc avascularity prevents the deposition of a provisional fibrin scaffold that typically facilitates soft tissue repair. Poor disc wound healing leads to disc damage accumulation and chronic inflammation characterized by overproduction of proinflammatory cytokines and proteolytic enzymes.
METHODS: Four lumbar IVDs from each of 31 Yucatan minipigs were randomized to untreated controls; degenerative injury (nucleotomy); and nucleotomy plus FS injection. Animals were killed at 1, 2, 3, 6, and 12 weeks postsurgery. IVDs were harvested to quantify (1) architecture using morphological and histological grading; (2) proteoglycan composition using DMMB assay; (3) cytokine content using ELISA; and (4) mechanical properties using quantitative pressure/volume testing.
RESULTS: There was progressive invasion of annular tissue into the nucleus of nucleotomy discs and concomitant reduction in proteoglycan content. By contrast, FS supplementation inhibited nuclear fibrosis and facilitated proteoglycan content recovery over time. FS discs synthesized significantly less TNF-α than degenerate discs (66% vs. 226%, P < 0.05) and had upregulation of IL-4 (310% vs. 166%) and TGF-β (400% vs. 117%) at 2 to 3 weeks posttreatment. At the third week postsurgery, the denucleated discs were less stiff than controls (pressure modulus 779.9 psi vs. 2754.8 psi; P < 0.05) and failed at lower pressures (250.5 psi vs. 492.5 psi; P < 0.05). The stiffness and leakage pressure of the FS-treated discs recovered to control values after 6 and 12 weeks, respectively.
CONCLUSION: FS facilitated structural, compositional, and mechanical repair of the surgically damaged IVD. These FS-derived benefits are likely due to its conductive scaffold properties and metabolically active constituents such as thrombin, factor XIII, and aprotinin acetate.
Fibrin Injection Stimulates Early Disc Healing in the Porcine Model
BACKGROUND CONTEXT: Pathologic disc degeneration includes ineffective healing of tissue damage that accumulates over time. Regions of inflammation, neoinnervation, and nociceptor sensitization can lead to chronic discogenic pain. An important component of normal wound healing occurs when fibrin interacts with matrix and cellular structures. The biostimulatory effects of fibrin include fibroblast recruitment, matrix synthesis, and granulation tissue formation. The Biostat Disc Augmentation System has been developed as a fibrin-based treatment for discogenic pain.
Fibrin in Intervertebral Disc Tissue Engineering
Alessandra Colombini1, Cristina Ceriani, Giuseppe Banfi, Marco Brayda-Bruno, Matteo Moretti
Affiliation:1
1
1 Laboratory of Experimental Biochemistry and Molecular Biology, IRCCS Galeazzi Orthopaedic Institute , Milan, Italy .
PMID: 24961887 DOI: 10.1089/ten.TEB.2014.0158
Abstract
Fibrin is clinically employed as a versatile, safe, and clinically applicable sealant and cell carrier. It has been able to support disc cell survival, favor extracellular matrix production, and enhance the efficiency of cell transfer in the intervertebral disc (IVD). The aim of this review was to evaluate how fibrin has been used in vitro, in vivo, and in clinical trials for IVD tissue engineering. Within the in vitro studies, disc cells were cultured in fibrin alone or combined with other materials and a difference in the behavior of nucleus pulposus (NP) and annulus fibrosus (AF) cells was sometimes reported, but in general, the formation of fibrocartilaginous matrix was observed. Moreover, data concerning the fibrin long-term stability and its anti-inflammatory properties were found. Disc cells of human origin were never employed in combination with fibrin in vivo or in clinical trials. In vivo, disc degeneration models used to test the fibrin properties essentially involved NP injuries. The addition of cells, in particular if terminally differentiated, to the injected fibrin seemed to promote a more physiological matrix in comparison with fibrin alone. Important aspects should be further investigated in future studies such as the use of fibrin to treat AF lesions as well as the mechanical properties of the fibrin-based biomaterials and of the neoformed tissue. Finally, in vivo studies and clinical trials with in situ injection of fibrin and human disc cells should be performed.
In vitro characterization and in vivo behavior of human nucleus pulposus and annulus fibrosus cells in clinical-grade fibrin and collagen-enriched fibrin gels
Alessandra Colombini1, Silvia Lopa, Cristina Ceriani, Arianna B Lovati, Samantha J Croiset, Alessia Di Giancamillo, Giovanni Lombardi, Giuseppe Banfi, Matteo Moretti
1). Affiliations
PMID: 25236589 DOI: 10.1089/ten.TEA.2014.0279
Abstract
The intervertebral disc (IVD) presents a limited self-repair ability and cell-based therapies have been suggested to prevent or treat IVD lesions. Fibrin-based scaffolds as cell carriers are promising candidates in IVD tissue engineering, thanks to their ability to be easily delivered into the defect and to adapt to the lesion shape, to support/retain the injected cells into the implantation site and to favor the production of a suitable extracellular matrix (ECM). We evaluated the in vitro and in vivo behavior of human nucleus pulposus (NP) and annulus fibrosus (AF) cells in a clinical-grade collagen-enriched fibrin that has never been tested before for orthopedic applications, comparing it with clinical-grade fibrin. The survival of IVD cells seeded within fibrin or collagen-enriched fibrin and the ECM synthesis were evaluated by biochemical, immunohistochemical, and transcriptional analyses, prior and after subcutaneous implantation of the gels in nude mice. After 28 days of implantation, NP and AF cells were still detectable within explants, produced tissue-specific ECM, and showed a higher content of glycosaminoglycans (GAGs) and type I and II collagen compared to gels before implantation. Both the fibrin gels, enriched or not with collagen, seemed to be suitable for the culture of AF cells, being able to support the homogeneous synthesis of type I collagen, characteristic of the native fibrocartilaginous AF tissue. Differently, fibrin alone was a more suitable matrix for NP culture, supporting the homogeneous deposition of GAGs and type II collagen. In conclusion, our results suggest to combine AF cells with fibrin, enriched or not with collagen, and NP cells with fibrin alone to maintain the typical features of these cell populations, indicating these clinical-grade materials as viable options in cell-based treatments for IVD lesions.
Fibrin promotes proliferation and matrix production of intervertebral disc cells cultured in three-dimensional poly(lactic-co-glycolic acid) scaffold
Abstract
Previously, we have proven that fibrin and poly(lactic-co-glycolic acid) (PLGA) scaffolds facilitate cell proliferation, matrix production and early chondrogenesis of rabbit articular chondrocytes in in vitro and in vivo experiments. In this study, we evaluated the potential of fibrin/PLGA scaffold for intervertebral disc (IVD) tissue engineering using annulus fibrosus (AF) and nucleus pulposus (NP) cells in relation to potential clinical application. PLGA scaffolds were soaked in cells-fibrin suspension and polymerized by dropping thrombin-sodium chloride (CaCl(2)) solution. A PLGA-cell complex without fibrin was used as control. Higher cellular proliferation activity was observed in fibrin/PLGA-seeded AF and NP cells at each time point of 3, 7, 14 and 7 days using the MTT assay. After 3 weeks in vitro incubation, fibrin/PLGA exhibited a firmer gross morphology than PLGA groups. A significant cartilaginous tissue formation was observed in fibrin/PLGA, as proven by the development of cells cluster of various sizes and three-dimensional (3D) cartilaginous histoarchitecture and the presence of proteoglycan-rich matrix and glycosaminoglycan (GAG). The sGAG production measured by 1,9-dimethylmethylene blue (DMMB) assay revealed greater sGAG production in fibrin/PLGA than PLGA group. Immunohistochemical analyses showed expressions of collagen type II, aggrecan core protein and collagen type I genes throughout in vitro culture in both fibrin/PLGA and PLGA. In conclusion, fibrin promotes cell proliferation, stable in vitro tissue morphology, superior cartilaginous tissue formation and sGAG production of AF and NP cells cultured in PLGA scaffold. The 3D porous PLGA scaffold-cell complexes using fibrin can provide a vehicle for delivery of cells to regenerate tissue-engineered IVD tissue.
Incorporation of Collagen and Hyaluronic Acid to Enhance the Bioactivity of Fibrin-Based Hydrogels for Nucleus Pulposus Regeneration
Affiliations
1Trinity Centre for Bioengineering, Trinity Biomedical Sciences Institute, Trinity College Dublin, 2 Dublin, Ireland. [email protected].
2School of Engineering, Trinity College Dublin, 2 Dublin, Ireland. [email protected].
3Trinity Centre for Bioengineering, Trinity Biomedical Sciences Institute, Trinity College Dublin, 2 Dublin, Ireland. [email protected].
4School of Engineering, Trinity College Dublin, 2 Dublin, Ireland. [email protected].
5Advanced Materials and Bioengineering Research (AMBER) Centre, Royal College of Surgeons in Ireland & Trinity College Dublin, 2 Dublin, Ireland. [email protected].
- PMID: 29996555
- PMCID: PMC6164980
- DOI: 10.3390/jfb9030043
Free PMC article
Abstract
Hydrogels, such as fibrin, offer a promising delivery vehicle to introduce cells into the intervertebral disc (IVD) to regenerate damaged disc tissue as a potential treatment for low back pain. However, fibrin lacks key extracellular matrix (ECM) components, such as collagen (Col) and hyaluronan (HA), normally found in native nucleus pulposus (NP) tissue. The overall aim of this work was to create a fibrin-based hydrogel, by incorporating Col and HA into the matrix to enhance NP-like matrix accumulation using articular chondrocytes (CC). Firstly, we assessed the effect of fibrin concentrations on hydrogel stability, and the viability and proliferation kinetics of articular chondrocytes. Secondly, we investigated the effect of incorporating Col and HA to enhance NP-like matrix accumulation, and finally, examined the influence of various HA concentrations. Results showed that increasing fibrin concentration enhanced cell viability and proliferation. Interestingly, incorporation of HA promoted sGAG accumulation and tended to suppress collagen formation at higher concentrations. Taken together, these results suggest that incorporation of ECM components can enhance the bioactivity of fibrin-based hydrogels, which may help advance the clinical potential of commercial cell and biomaterial ventures in the treatment of IVD regeneration.
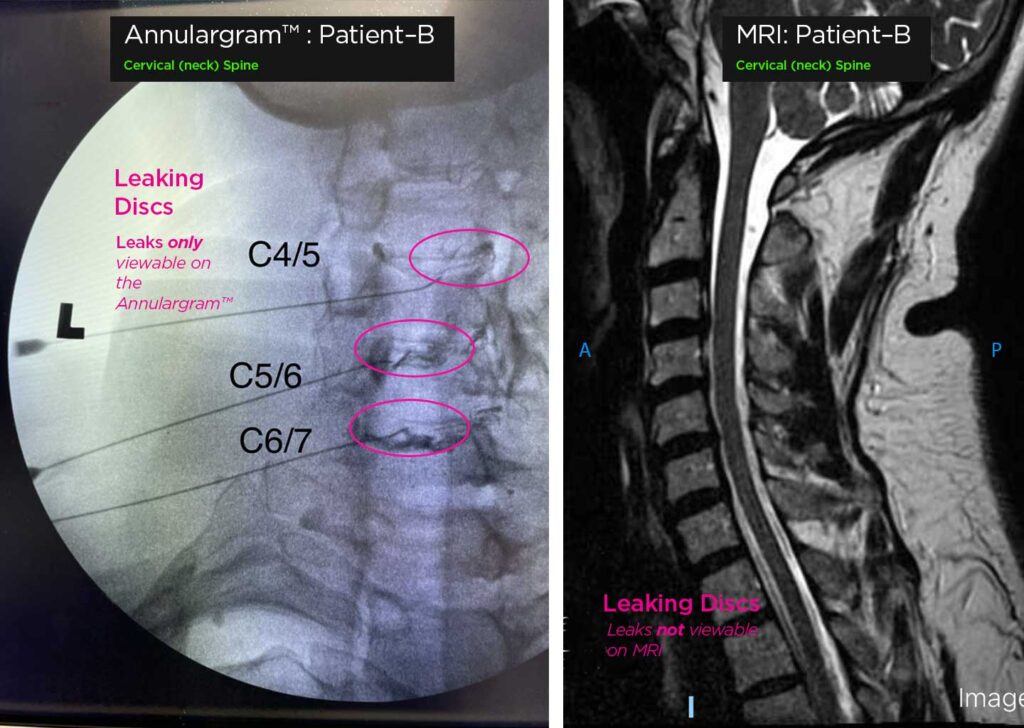
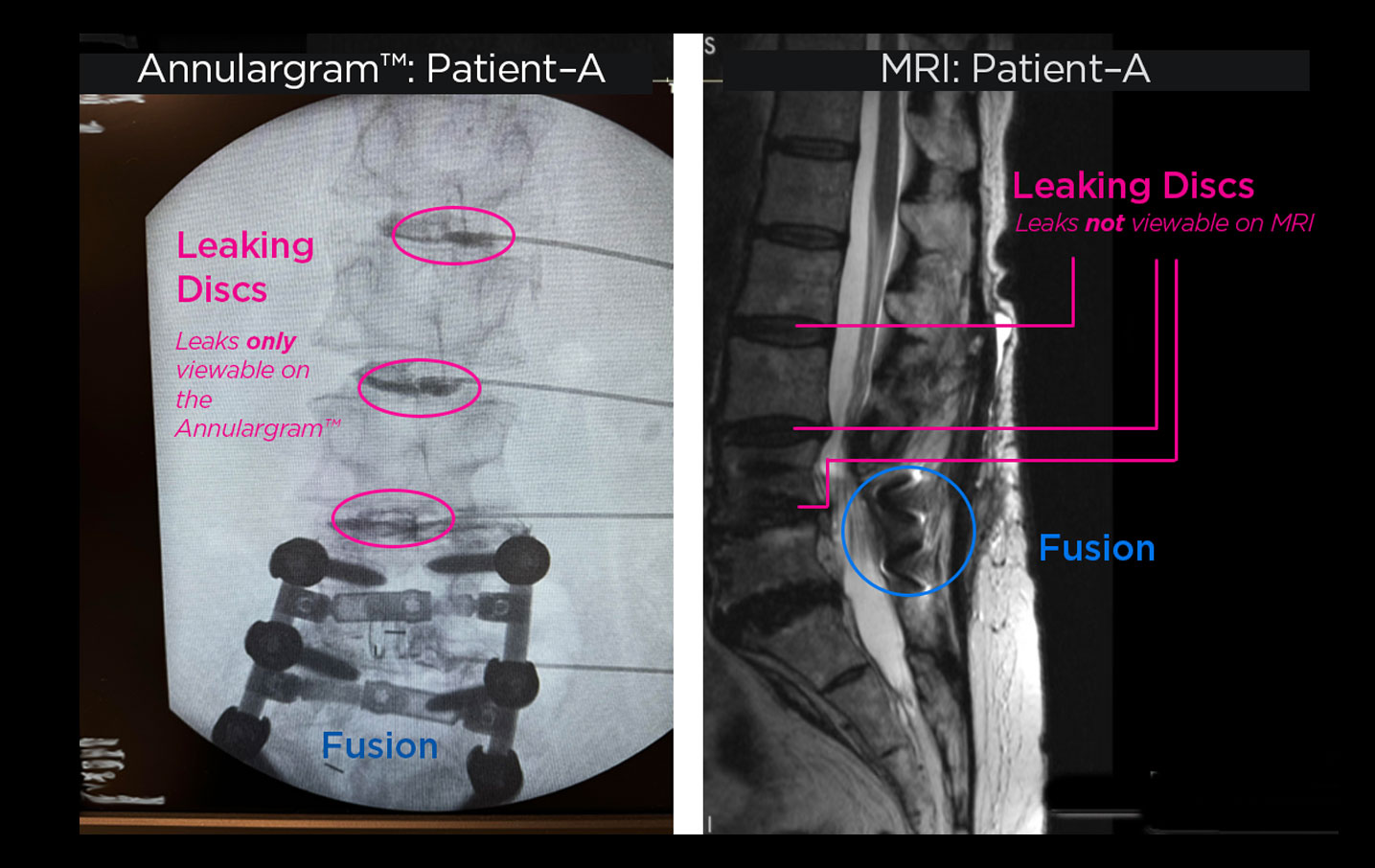
The Annulargram™ and MRI comparison
Comparison of Lumbar spine Annulargram™ and Lumbar Spine MRI . As shown: leaky discs are only visible on the Annulargram™